| Key
Facts |
- Accumulation of
abundant protein rich and lipid rich material resembling surfactant
in alveoli
- Radiographically,
bilateral symmetric central airspace opacities or vague hazy opacities,
perihilar and in lower lungs
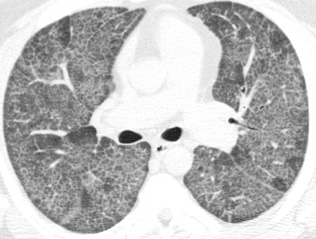
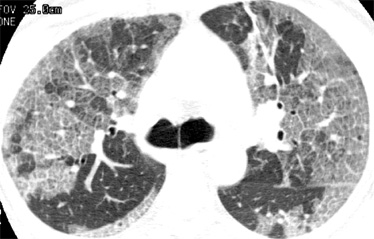
- HRCT shows a “crazy-paving”
appearance
- A third of patients
are asymptomatic
- Occurs with massive
silica dust exposure
- Associated with
infections such as Nocardia
- Diagnosed and treated
with BAL and irrigation
- Good prognosis
|
| Imaging
Findings |
Chest
radiograph
- Ill-defined nodular,
or diffuse airspace opacification or vague ill-defined opacities
- Central perihilar
batwing pattern
- Mixed interstitial
and airspace opacities, less common
CT/HRCT
- HRCT shows geographic
regions of airspace or ground glass opacities and linear interstitial
opacities, giving a “crazy-paving” pattern.”
- Distribution of
disease is random.
|
| Differential
Diagnosis |
- Pulmonary edema
- Pneumonia
- Hemorrhage
- Bronchioloalveolar
cell carcinoma
- Differentiation
- No cardiomegaly,
pulmonary venous hypertension or effusions
- Pneumonia and
hemorrhage can be excluded by clinical presentation and bronchoscopy
- Crazy-paving
can also be seen in bronchioloalveolaar carcinoma, lipoid pneumonia,
hemorrhage, pulmonary edema and bacterial pneumonia
|
| Pathological
Features |
- Accumulation of
abundant protein rich and lipid rich material resembling surfactant
- Alveoli are filled
with fine granular material that stains pink with PAS stain
- Abnormality of
surfactant production, metabolism or clearance by type II alveolar cells
and macrophages
- Often superinfected
with infections with Nocardia, Aspergillus, Cryptococcus and other organisms.
|
| Clinical
Presentation |
- Uncommon
- Adults 20 to 50
years olds
- >2:1 male predominance
- Can occur in very
young children
- Can occur with
exposure to high concentrations of silicon dioxide dust or titanium
- Can occur in immuno-compromised
children, or adults with lymphoma, leukemia, AIDS, or autoimmune disease
- Chest radiograph
is abnormal out of proportion to patient’s symptoms
- 33% are asymptomatic,
most common symptoms are dyspnea and cough
- Clubbing of fingers
and toes
- Diagnosis with
BAL or transbronchial biopsy
- Treatment, therapeutic
BAL with whole lung irrigation, usually one to two times. Few patients
require annual or biannual therapeutic BALs.
- Prognosis is good.
- Death from pulmonary
fibrosis is rare.
|
| References |
Murch
CR , Carr DH. Computed tomography appearances of pulmonary alveolar proteinosis
Clin Radiol 40:240-243, 1989
Gale ME, Karlinsky JB , Robins AG. Bronchopulmonary lavage in pulmonary
alveolar proteinosis: chest radiograph observations AJR Am J Roentgenol
146:981-985, 1986
Prakash UB, Barham SS, Carpenter HA, et al. Pulmonary alveolar phospholipoproteinosis:
experience with 34 cases and a review Mayo Clin Proc 62:499-518, 1987
|