| Key
Facts |
- Subacute or chronic
inflammatory polyarthropathy of unknown cause
- Thoracic involvement
more common in males
- Major findings
are pleural disease, interstitial fibrosis with honeycombing, micronodules,
small and large nodules, and airway disease
- HRCT useful to
show character and extent of pleuropulmonary and airway disease (obliterative
bronchiolitis, BOOP, follicular bronchiolitis, bronchiectasis)
- Interstitial lung
disease can be UIP or NSIP, the latter having a better prognosis
- Treatment - steroids
and immunosuppressive drugs
- Complications include
pneumonia, empyema, drug reaction, amyloid, cor pulmonale
|
| Imaging
Findings |
Chest
radiography
Pleural Disease
- Pleural thickening
(20%)
- Pleural effusion,
mostly in males (3%)
- Small to
large
- Usually unilateral,
can be bilateral
- Transient,
persistent or relapsing
- Fibrothorax
- Susceptible
to empyema
- Pneumothorax
- rare
Parenchymal Disease
- Reticulonodular
and irregular linear opacities, lower zones (<10%)
- Distortion, honeycombing,
progressive loss of volume
- Upper lobe fibrobullous
disease, rare
- Rheumatoid nodules,
rare
- Solitary
or multiple
- 5 mm to 7cm
- Peripheral
- Wax and wane
- May cavitate,
thick smooth wall
- May calcify
- Caplan’s
syndrome – rare
- Hypersensitivity
reaction to dust
- Coal miners,
rheumatoid arthritis, large rounded nodules (0.5 to 5 cm)
- Redefined
to include
- Silica,
asbestos, dolomite, carbon
- Serologic
and not clinical RA
Airway Disease
- Obliterative
Bronchiolitis - normal or hyperinflation
- BOOP –
same as idiopathic BOOP
- Follicular bronchiolitis
– diffuse reticulonodular pattern
- Bronchiectasis
- Upper airway
disease
CT/HRCT
Pleural Disease
- most common
- Pleural thickening
or effusion
- May be associated
with pericarditis, interstitial fibrosis, interstitial pneumonia or
lung nodules
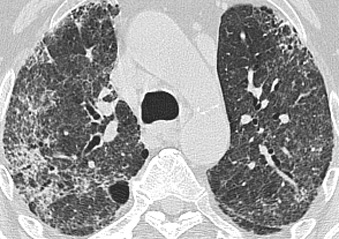
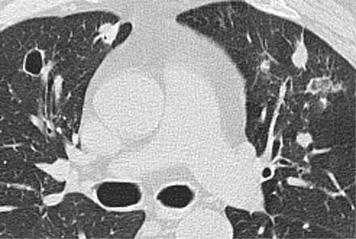
Parenchymal Disease
- Pulmonary fibrosis
indistinguishable from UIP,
- Basilar and
peripheral progresses in some to diffuse and central
- Intralobular
lines, irregular thickened interlobular septa
- Honeycombing
(10%), mostly at bases, distortion
- Ground glass
opacities (14%)
- Consolidation
(6%)
- Nodules (22%)
– micronodules (centrilobular, peribronchial, subpleural)
- Nodules/masses
- Resemble
neoplasm, discrete, rounded or lobulated, subpleural.
Airway Disease
- Obliterative
Bronchiolitis – mosaic pattern, bronchiectasis
- BOOP –
see idiopathic BOOP
- Follicular bronchiolitis
– nodules < 1 cm; centrilobular, subpleural, peribronchial;
centrilobular branching pattern
- Bronchiectasis
- Upper airway
disease
Other findings
- Cor pulmonale,
lymphadenopathy, sclerosing mediastinitis, pericarditis
|
| Differential
Diagnosis |
- Lung
- IPF
- Scleroderma
- Asbestosis
- Drug Reaction
- BOOP
- Hypersensitivity
pneumonitis
- Pleural
- Metastases
- Empyema
- Mesothelioma
- Hemothorax, old
- Empyema, old
- Differentiation
- Hand films,
changes of RA
- Chest x-ray:
erosion of distal clavicles
|
| Pathological
Features |
|
|
| Clinical
Presentation |
- RA is 3x more common
in females,
- Extraarticular
RA - more common in males, age 50-60 years
- Thoracic disease
may develop before, at onset or after onset of arthritis
- Insidious onset,
relapses and remissions
- Asymptomatic, or
dyspnea, cough, pleuritic pain, finger clubbing, hemoptysis, infection,
bronchopleural fistula, pneumothorax
- Most have arthritis;
positive rheumatoid factor (80%), and cutaneous nodules
- Pleural fluid -
high protein, low glucose, low pH, high LDH, high RF, low complement
- PFTs - restrictive
defect, reduced diffusing capacity, sometimes obstructive defect
- Treatment
- Steroids
- Iimmunosuppresant
drugs
- Variable prognosis,
5 year survival 40%
- Death from
infection, respiratory failure, cor pulmonale, amyloid
|
| References |
Turner-Warwick
M , Evans RC. Pulmonary manifestations of rheumatoid disease Clin Rheum
Dis 3:549-564, 1977
Remy-Jardin M, Remy J, Cortet B, et al. Lung changes in rheumatoid arthritis:
CT findings Radiology 193:375-382, 1994
|