| Key
Facts |
- Pneumoconiosis
from fibrous silicate minerals
- Peripheral lower
zone irregular opacities
- 25% have associated
pleural plaques
- HRCT
- Subpleural
curvilinear lines
- Interlobular
lines (Short) and parenchymal (long) lines
- Centriacinar
nodules (peribronchial firbrosis)
|
| Imaging
Findings |
Chest
Radiograph
- May be normal
- Peripheral lower
zone predominance
- Irregular reticular
opacities
- ILO classification:
s,t,u opacities
- Late: end-stage
honeycombing
- May have pleural
plaques (25%)
- Lung cancer: lower
zone predominance
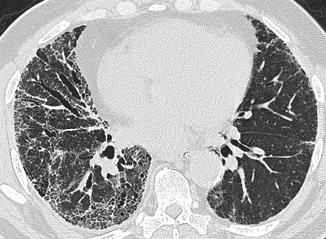
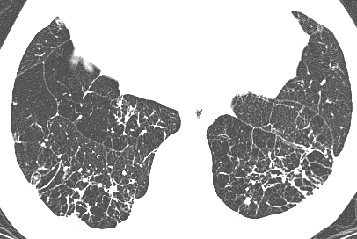
CT/HRCT
- More sensitive
than chest radiograph
- Interlobular septal
thickening (short lines)
- Subpleural lines
- Parenchymal bands
- Centriacinar nodules
(peribronchial fibrosis)
- Honeycombing
- Ground glass opacities
- Atelectasis (reversible
prone position)
|
| Differential
Diagnosis |
- Idiopathic pulmonary
fibrosis
- Scleroderma
- Rheumatoid arthritis
- Hypersensitivity
pneumonitis
- Lymphangitic tumor
- Cytotoxic drug
reaction
|
| Pathological
Features |
- Fibrosis + asbestos
bodies equals asbestosis
- 2 types of fibers
- Serpentine
(chrysotile, 90% commercial asbestos)
- Curly,
wavy fiber
- Long (>100
µm)
- Diameter
(20 – 40 µm)
- Amphibole (amosite,
crocidolite)
- Straight,
rigid fiber
- Variable
length diameter
- Aspect
ration (length/width) > 3:1
- Retention: long
thin fibers > short thick fibers
- Asbestos (Ferruginous)
bodies
- Hemosiderin
coated fiber (mostly amphibole)
- Incompletely
phagocytized by macrophages
- Not pathognomonic
for asbestosis
- Coated fibers
< uncoated fibers
- Not correlated
with fibrosis
- Early fibrosis:
centered on respiratory bronchioles
- Patchy distribution
- Fibrosis associated
with > 1 million fibers/gm lung tissue
- Honeycombing: subpleural
distribution
|
| Clinical
Presentation |
- Mills, insulation,
shipyards, construction
- Latent period 20-30
years
- Multiplicative
risk factor for lung cancer
- Clinical diagnosis
(4 of 5 criteria)
- Exposure history
- Dyspnea on
exertion
- Inspiratory
crackles
- Abnormal compatible
chest radiograph
- Restrictive
pattern pulmonary function
- No treatment, stop
smoking, consider lung cancer screening
- Most die lung cancer
|
| References |
Aberle
DR , Balmes JR. Computed tomography of asbestos-related pulmonary parenchymal
and pleural diseases Clin Chest Med 12:115-131, 1991
Akira M, Yokoyama K, Yamamoto S, et al. Early asbestosis: evaluation with
high-resolution CT Radiology 178:409-416, 1991
|